

Introduction: Central nervous system (CNS) relapse occurs in 2-10% of patients with diffuse large B cell lymphoma (DLBCL) and carries a poor prognosis. The CNS-IPI score identifies patients at high-risk (10-12%) of CNS relapse based on the presence of 4-6 risk factors: age >60 years, ECOG performance status >1, elevated LDH, stage III to IV, >1 extranodal site, and renal or adrenal involvement. International guidelines recommend prophylactic intravenous high-dose methotrexate (HD-MTX) for patients at high-risk of CNS relapse. However, there is limited evidence supporting this practice, and prophylactic HD-MTX requires hospital admission and increases the risk of treatment-related toxicity. Therefore, we conducted a real-world study to determine the effectiveness of HD-MTX for prevention of CNS relapse in high-risk DLBCL.
Methods: We performed retrospective chart reviews of patients aged 18-70 years with DLBCL treated with curative intent at two academic medical centers in Alberta, Canada between 2012-2019. Since 2015, the Alberta Provincial Lymphoma Clinical Practice Guideline (APLCPG) has recommended CNS prophylaxis with HD-MTX 3.5g/m2 IV after cycles 2, 4, and 6 of R-CHOP for patients with the following high-risk criteria: CNS-IPI 4-6, double hit lymphoma, or testicular involvement. Between 2012-2015, HD-MTX was recommended for patients with elevated LDH, ECOG >1, and >1 extranodal site. In addition, eligible patients at risk of poor outcomes (e.g. double hit lymphoma or IPI score 4-5) could be offered higher intensity chemoimmunotherapy (e.g. da-EPOCH-R or R-CODOXM/R-IVAC) or R-CHOP followed by consolidative autotransplant. The log-rank test was applied to determine risk of CNS relapse and the Cox proportional-hazards model was used to determine factors associated with CNS relapse, progression-free survival (PFS), and overall survival (OS). Analyses were performed using SPSS version 25 and GraphPad Prism 8 statistical software.
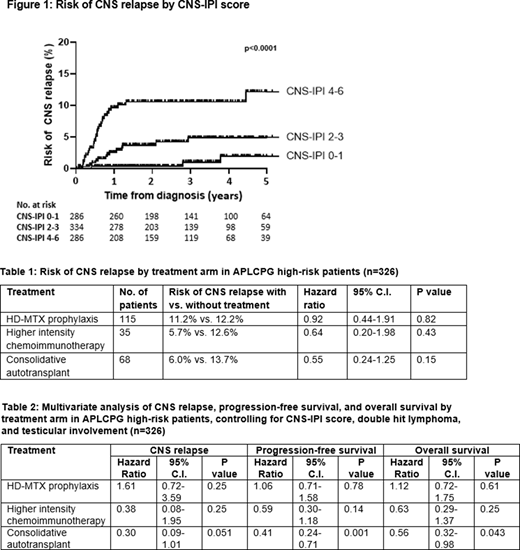
Results: We included 906 patients with a median follow-up time of 35.3 months (range 0.29-105.7). Risk of CNS relapse was 1.9% (95% C.I. 0.0-30.7%) for patients with CNS-IPI 0-1, 4.9% (95% C.I. 0.5-18.0%) for CNS-IPI 2-3, and 12.2% (95% C.I. 4.0-25.2%) for CNS-IPI 4-6 (p<0.0001). Risk factors for CNS relapse included APLCPG high-risk criteria (HR 4.69, 95% C.I. 2.51-8.76), CNS-IPI score 4-6 (HR 4.26, 95% C.I. 2.22-8.16), and testicular involvement (HR 3.45, 95% C.I. 0.43-27.34). Among the 326 patients meeting APLCPG high-risk criteria, median CNS-IPI was 4 (range 0-6), 67 (20.6%) had double hit lymphoma, and 17 (5.2%) had testicular involvement. Risk of CNS relapse was significantly increased for patients meeting APLCPG high-risk criteria (11.8% vs 3.0%, p<0.0001). Prophylactic HD-MTX was administered to 115 (35.3%) high-risk patients; median number of doses given was 2 (range 1-3). The risk of CNS relapse was 11.2% (95% C.I. 2.1-28.9%) for patients who received HD-MTX versus 12.2% (95% C.I. 2.8-28.8%) for those who did not (p=0.82). Patients who underwent higher intensity chemoimmunotherapy (n=35) or consolidative autotransplant (n=68) tended to have a lower risk of CNS relapse than patients treated with conventional R-CHOP (6.0% vs. 14.6%, p=0.09). In multivariate analyses, HD-MTX and higher intensity chemoimmunotherapy demonstrated no significant association with CNS relapse, PFS, or OS; however, consolidative autotransplant was associated with a tendency toward lower risk of CNS relapse (HR 0.30, 95% C.I. 0.09-1.01) and a significantly improved PFS (HR 0.41, 95% C.I. 0.24-0.71) and OS (HR 0.56, 95% C.I. 0.32-0.98).
Conclusion: The APLCPG high-risk criteria of CNS-IPI 4-6, double hit lymphoma, or testicular involvement identify patients with DLBCL at significantly increased risk of CNS relapse. The risk of CNS relapse was similar for all high-risk patients (11.8%) and those who received prophylactic HD-MTX (11.2%) in our study relative to previously published data for patients who did not receive CNS prophylaxis (10-12%). Based on this analysis, we could not demonstrate a benefit to the current practice of prophylactic HD-MTX. However, the lower rate of CNS relapse and improved PFS and OS in patients who received consolidative autotransplant in our study suggests that optimizing frontline therapy to achieve better systemic disease control may be a more effective strategy to reduce the risk of CNS relapse than prophylactic HD-MTX alone.
Stewart:Teva: Honoraria; Sandoz: Honoraria; Novartis: Honoraria; AstraZeneca: Honoraria; Amgen: Honoraria; Roche: Honoraria; Janssen: Honoraria; Abbvie: Honoraria; Gilead: Honoraria; Celgene: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal